We often receive questions about various surgical interventions that are often indicated after facial palsy to help overcome complications and residuals. So, we would like to discuss what you can expect from some of the most popular surgeries performed for Bell’s palsy and in which cases they might be indicated.
At Crystal Touch, we follow a non-invasive recovery approach, that is applicable to most cases of peripheral facial palsy. The purpose of this article is to provide you with our professional opinion and information, so you can make an informed decision.
Estimated reading time: 23 minutes
You can watch the video below or read the full article under it.
Table of contents
First, let’s take a look at two surgical interventions that are usually indicated during the acute stage of Bell’s palsy: Tarsorrhaphy and insertion of gold or titanium weights.
Tarsorrhaphy
Tarsorrhaphy is the procedure of sewing together corners of the eye on the side of the face affected by Bell’s palsy.
The purpose is to protect the eye from drying out during the acute phase, when the eye does not close and the tear production is impaired. If the eye stays dry, it can damage the cornea of the eye.
When it can be indicated
This surgery is not indicated very often. There are also some non-invasive alternatives that can provide sufficient protection for your eye:
- a moisture chamber,
- an eye patch,
- artificial tears.
A moisture chamber is a transparent protective plate with pores, that is glued to your eye socket and protects it from drying out, while still allowing it to breathe. It can be worn for as long as needed.
An eye patch can be used only at night or also during the day, to help keep your eye closed and safe.
If your eye does close, so it can be protected from dust, but there are simply not enough tears, you can use artificial tears to keep your eye moist throughout the day and wear an eye patch at night.
Insertion of golden weight
Another surgery that can be performed to protect the eye during acute Bell’s palsy is the insertion of golden or titanium weights into the upper eyelid. The idea is that the weight will assist your eyelid in closing. After, when the assistance is no longer needed, the weights are removed from the eyelid.
When it can be indicated
This surgery is also not used very often anymore, but it is still sometimes indicated. Whether it is efficient, needs to be considered. On the one hand, when the weight is pushing down, it helps to close the eye. On the other hand, to open the eyelid, you need a much higher effort from the Levator Palpebrae Superioris – the little muscle that opens the eyelid. This means that the muscle becomes stronger, as it needs to lift up higher weight to open the eye every time. As a result, the muscle becomes more difficult to relax and stretch, which leads to more difficult blinking even after the weights are removed.
Blepharoplasty
During blepharoplasty for Bell’s palsy, the upper or lower eyelid is surgically affected so that the eye becomes visually larger or smaller. It is sometimes indicated 3 – 4 months or even a year after Bell’s palsy.
When it can be indicated
At Crystal Touch, our opinion is that Blepharoplasty after facial palsy is not very necessary, except for some extreme cases. Our opinion is based on the fact that the irregularities in the closure of the eye and visibly smaller eye fissure are related to the function of one particular muscle – Levator Palpebrae Superioris – and not to physical or anatomical differences between the healthy and affected side.
Levator Palpebrae Superioris is a muscle that lifts up the eyelid. Although this muscle serves the eyelid – opening and closing it – it does not belong to the facial nerve. It is innervated by the third cranial nerve, Nervus Oculumotorius. The same nerve provides for the movement of the eyeballs. If you look down with just your eyes, without moving your head, you will see that your eyelid also goes down, without any effort from your side. If you have synkinesis, it will not be present in this movement. That is because the signal is directed through the third cranial nerve, and not through the facial nerve that was affected by Bell’s palsy.
This illustration shows that except for very few extreme cases, this muscle can be affected by non-invasive methods and the eye fissure can be regulated without surgery. All that is needed is a specific rehabilitation that focuses on adjusting the eye fissure.
Muscle Transposition
This surgical intervention for Bell’s palsy also has been popular some years ago. During Muscle Transposition, the flap of the temporal muscle is taken, reversed, and connected to the mouth corner. As a result, the affected mouth corner would go up when the person imitates chewing by clenching the teeth together. This is performed only on the affected side of the face.
When it can be indicated
From our experience, this operation is indicated only in the cases when it is absolutely certain that the facial nerve, at least its zygomatic branch which connects the brain with the muscles that provide for the smile, is absolutely, 100%, dead. This happens very, very rarely. It is extremely seldom when during Bell’s palsy, Ramsay Hunt Syndrome, and any other non-injury, non-surgical facial palsies, the facial nerve might be damaged irreversibly.
An example of when this surgery might be indicated is the removal of a tumour of the parotid gland. If the parotid gland had to be removed, with that operation, the respective zygomatic branch had to be cut through and becomes irreversibly damaged. Then one may consider this surgical intervention as otherwise, the mouth corner will be completely motionless. Because there are no signals that can pass through the permanently severed nerve branch.
If this is something you are considering, you need to be very realistic in your expectations. This is a rather radical intervention. It involves a part of a muscle that is five-six millimetres wide. It is physically sewn to your moth corner. So there will be a little bulge, and it is not necessarily that it will work perfectly as we may expect or may be promised. It is a rather sensitive matter and I suggest that you very seriously consider, and read all possible sources. Talk to people who have had this experience, because once it is done, it cannot be undone.
Nerve Graft
Nerve Graft is an operation when part of your nerve is being taken (usually) from your lower leg, and then your healthy side is connected to your affected side across the face.
In the illustration, the red line indicates the way the nerve graft is connected from the healthy side to the affected. The red dot indicates the approximate site of connection.
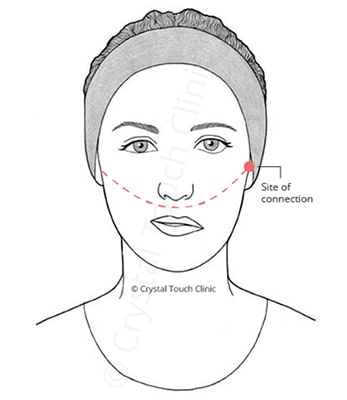
What the Nerve Graft operation involves
To perform the nerve graft, the surgeon will cut out a piece of the nerve (usually from the calf muscle) and insert it into the facial tissue in order to connect the facial nerve branch on the healthy side to the respective branch on the affected side.
In most cases, the nerve graft operation is performed to reinnervate the facial muscles that are involved in smiling. To do that, the stem of the facial nerve branch that usually provides those signals to the affected side needs to be severed. This process irreversibly blocks the transmission of signals via the affected facial nerve branch. So if there was any possibility to recover the nerve using natural methods, it becomes obsolete. Once the nerve branch is cut in preparation for the nerve graft, it cannot be restored.
The only signals that will be reaching the smile muscles on the affected side will be the signals produced for the healthy side that through the graft will travel to the affected side. However, everything is not that simple in real life.
This brings us to the second point. A human nerve is not like a wire. You can cut a wire in any spot, attach it to another wire and it will be conducting electrical signals. Once you cut any nerve branch, all nerve fibres inside of it will degenerate. The only thing that will be left is the hollow tubes made of connective tissue that serve as a protective passageway for the nerve fibres to regenerate and eventually reach their destination.
The prepared nerve graft is then connected from the healthy side to the affected side (red line on the illustration). The nerve fibres from the healthy side have to grow within the hollow tubes to connect with the nerve branch on the affected side and grow further until they reach the smile muscles (blue line).
That is a very long way to grow.
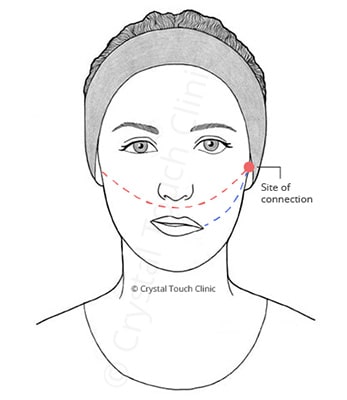
Our facial nerve fibres can grow at a maximum of 1 mm per day, in the most optimal conditions. In this case, the facial nerve has to grow approximately 15 to 20 cm until the connection site and then another 5 to 6 cm to the muscles. That is more than 200 days of waiting. There is also a fair chance that a considerable part of those nerve fibres that are growing will stop regenerating on the way and will not reach their destination muscles.
That is why in Nerve Graft it is difficult to predict with certainty the results.
When it can be indicated
In our opinion, it should be indicated only in cases where the facial nerve trunk has been irreversibly injured, just like in the case of Muscle Transposition.
Selective Neurolysis
What is Selective Neurolysis? ‘Lysis’ is destruction. ‘Neurolysis’ is the destruction of the nerve. Selective Neurolysis is a selective destruction of the nerve.
During Selective Neurolysis the surgeon cross-secs some of the fibres of the facial nerve that provide signals from the brain to the ‘unwanted’ muscles. In most cases, it is the muscle that is called Depressor Anguli Oris – a muscle that pulls down the mouth corner.
After facial palsy, this muscle often stands in the way of a smile, by contracting simultaneously with Zygomatic muscles that try to pull the mouth corner up. This muscle becomes active and like an antagonist, pulls the mouth corner down. As a result, the mouth corner does not move or even points downwards.
In order to reduce this resistance, a surgeon cuts some nerve fibres going towards the Depressor Anguli Oris to reduce its pulling power. As a result, the smile often gets better.
When it can be indicated
Selective Neurolysis is mainly indicated or suggested in the cases when the patient is experiencing synkinesis. Synkinesis is involuntary contractions of certain facial muscles, which do not belong to the intended facial movement. We discuss it in more detail in the article “What is Synkinesis?”.
Whether to go for it? Yes or no? It is totally up to you. That depends on your preferences and your expectations, on your possibilities, on your reservations for the surgery. Although this is a minimal surgical intervention for Bell’s palsy, it is still an invasive solution, nonetheless, and it removes your chances for a natural recovery in the future. The area where this surgery is performed will be permanently denervated. Also, there is always a possibility that the result will not be as expected. It depends on your specific case, the surgeon’s skills and what you expect.
Botulinum Toxin
Another non-surgical, but still a little invasive intervention is Botulinum Toxin or Chemodenervation. It means that the nerve is being affected by chemical substances, in this case, Botulinum Toxin. The toxin is a poisonous substance which is produced by the bacteria Clostridium Botulinum that reside in the rotten meat. That is why it is called Botulinum Toxin – “sausage poison”.
Injections of botulinum toxin can be effective in the reduction of symptoms of synkinesis and bring some aesthetical improvement, but their effect is temporary. It produces a similar effect to Selective Neurolysis. It chemically damages the connection site between the facial nerve fibre and the muscle fibres, to reduce the signals going to specific muscles. As a result, this specific muscle will be contracting less. However, it only affects the symptoms and is not the cause of the irregular signal patterns that originate in the brain. So, it does not fix the problem, it only temporary masks its manifestations. After several weeks or months, the injections have to be repeated.
When it can be indicated
Just as Selective Neurolysis, Botulinum Toxin is usually indicated for patients with synkinesis. It can be done when you wish to see quick improvement, without having to go for more invasive options. However, it has to be repeated often and can become very costly. Also, it does not solve the problem, unlike a professional rehabilitation program, it simply reduces the symptoms.
Surgical considerations
Why do we believe that it is very important to consider all possible information before performing surgery? Because once performed, surgery cannot be undone. It often leads to unchangeable alterations to your facial nerve.
Surgery is forever
Surgery removes any future possibilities of natural recovery and improvement. If your facial nerve was physically damaged during a head injury in an accident or another surgery, such as being cut during the removal of a tumour, surgery can become the only hope for any improvement. This can also include some birth defects.
However, if your facial nerve sustained damage due to any peripheral facial palsy, such as classical Bell’s palsy, Ramsay Hunt Syndrome, or any other, we believe that there is a possibility for improvement with non-invasive methods. We have seen this in our patients, who came to us with complications after 10, 25, and 30 or more years since the onset of Bell’s palsy. We have also seen improvements in our patients with certain congenital facial palsies.
The results are difficult to predict
Second, the results of surgery may not be as expected, and you will have to live with it. Although most surgeons are very skilled in their work, our nerves and their recovery can be very unpredictable. Nerve fibres are more sensitive and difficult for our body to recover and reconstruct than muscular or other tissues. Any surgery for facial palsy will require nerve tissue recovery, and it cannot be predicted with certainty how this recovery will turn out. The more complicated is the surgery, the less guarantees can be made.
Therefore, we are certain that surgery should be considered only as the very last resort if all else led to no success, and you have lost all hope.







