Bell’s palsy is a diagnosis used to describe peripheral facial palsy. It is a sort of acute functional disorder. Bell’s palsy is essentially a diagnosis of exclusion for peripheral facial palsy. If the causes of your facial palsy cannot be determined and confirmed, the diagnosis will be “Bell’s palsy”.
Bell’s palsy can have numerous causes, including local over-cooling of face, head and neck area from cold weather, wind, air-conditioning, drafts. Additional risk factors are stress, hypertension and the last weeks of pregnancy. Bell’s palsy only affects your facial nerve and not your facial muscles. The damage results in the inability of the facial nerve to provide signals to your facial muscles. What you may experience as facial pains, contractures of facial muscles, tension, synkinesis and other discomforts after Bell’s palsy – are complications and residuals that develop during the long recovery period. They are not Bell’s palsy in itself, they are only the effects that develop because of the long recovery.
Let’s take a closer look at how Bell’s palsy affects the facial nerve and how it recovers over time.
Which parts of the facial nerve become damaged by Bell’s palsy?
There are five major branches in the facial nerve. They innervate various muscles of facial expressions. Most of the time, the damage to the facial nerve during Bell’s palsy happens in the narrow bone channel just behind the ear. This is the place where all five branches are still connected together in one “tube”.

The branches and the muscles they innervate:
• Temporal branch – forehead muscle, frown muscle, the upper part of circular muscle of the eye
• Zygomatic branch – the lower part of circular muscle of the eye, nasal muscles, the elevator of the upper lip muscle, zygomatic muscles
• Buccal branch – upper part of circular muscle of the mouth, elevator of the mouth corner, cheek muscle, risorius muscle
• Marginal mandibular branch – depressor of the mouth corner, depressor of the lower lip, chin muscle
• Neck branch – superficial neck muscle (platysma)
When Bell’s palsy occurs, all branches sustain damages from compression or disrupted blood supply to the trunk of the facial nerve. The regeneration speed of the damaged nerve fibres (axons) is not the same for all branches. For this reason, all the functions of facial muscles do not return at the same time. Sometimes the ability to close an eyelid may return first, in other cases it can be the mouth corner movements or the eyebrow lifting.
The three stages of damage to the facial nerve during Bell’s palsy
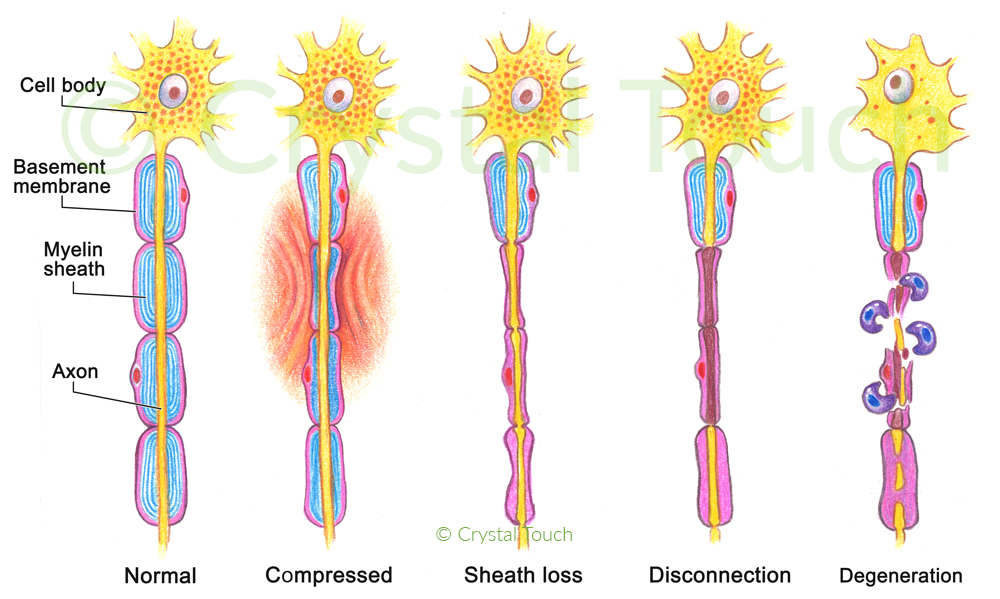
Stage 1: damage by compression or disruption of blood supply.
As we know from the previous article about the structure of the facial nerve, the nerve fibre (axon) is a living cell. Therefore, it is susceptible to damage by mechanical compression or from disruption of blood supply.
Bell’s palsy usually develops within several hours, sometimes within a couple of days. At this stage, it is crucial to put “all hands on deck” and fight the cause of the damage – viral infection, swollen tissue or vascular spasm.
Stage 2: development of a conduction block (sheath loss and disconnection).
Within the first 1-3 days of the nerve compression or ischemia, the Schwann cells that provide electrical insulation of the axon – die. Conduction of mimetic signals between the brain and facial muscles stops. This is called a “conduction block”. At this stage, the damage to the nerve is still minimal and if handled promptly, the new Schwann cells will regrow and restore the electrical insulation of axons. A complete spontaneous recovery in such cases can take place within 3 to 5 weeks.
Stage 3: axonal degeneration takes place (disconnection).
If the damaging factor persists longer than 4-6 days, the axon (conducting wire) dies, and axonal degeneration progresses. Now there is no physical connection between the brain and facial muscles any more. Axons have to regenerate all the way from cite of the damage to the facial muscles. On average, it is a distance of 9-10 cm. Under the best conditions, the speed of axonal regeneration happens at 1mm per day. So, it can take up to 3 months before the first facial movements reappear.
The recovery of the facial nerve after Bell’s palsy

As soon as the damage to the facial nerve has occurred, our body starts the regeneration process. It needs to re-grow about 7,000 axons (nerve fibres), and also recover their electrical insulation (myelin sheath). As soon as the axons begin to reconnect to the facial muscles, we start feeling slight twitching, itching, vibration or similar sensations. These are all good signs. Soon after that, the facial movements begin to come back.
Long before the normal mimetic movements reappear, the tone of the facial muscles returns. Then in the neutral state the face looks (almost) symmetrical. Asymmetry becomes clearly visible only during speech or emotions.
How long can regeneration of the facial nerve last after Bell’s palsy?
The nerve fibres grow rather slowly – no more than 1mm per day. Usually, you will start seeing the movements coming back within the 3 to 4 months during the onset. In some cases, it is likely to take longer time, if the damage was very severe. Sometimes the regeneration of certain nerve fibres stops half-way. They do not reconnect to their target muscles. Then, only part of the muscle regains its functions. This results in muscle weakness, and also in muscle contractures due to “overworking” of the few recovered fibres. There are some things that we can do in order to stimulate further the regeneration of these axons. We work on that with our patients during their rehabilitation programs.
Another complication of the slow recovery after Bell’s palsy is synkinesis. Synkinesis is the involuntary contraction of those facial muscles that are not normally involved in a particular mimetic movement. For example, involuntary closing of the eyelid during speech or while smiling. Another common synkinesis is the movement of the mouth corner as one blinks or squeezes the eyes. In our clinic we also work with our patients to reduce the manifestations of synkinesis.
Which movements are more likely to appear first?
It is hard to say, which movement will come back first. Often the closing of the eye and the small movements of the mouth corner return sooner than other muscles’ functions. From my experience, in most patients, the lifting of the eyebrow (forehead muscle) is the last one to recover. The reason for this is unknown to me.
What can we do to aid the recovery?
It is of great importance to do the GENTLE facial massages several times per day during the whole recovery period. This stimulates nerve regeneration and prevents contractures. We discuss more suggestions on what to do, what not to do and what to avoid in another post.







